
IVF and The Christian Worldview #1
IVF and The Christian Worldview #1
Technical Considerations

In 2021 after a year of trying to conceive naturally Sarah and I were forced to confront the difficulties of infertility and begin testing and treatment in our efforts to have bio children. After learning the underlying issues and trying several other methods of treatment, IVF became the last option available to us. The emotional and mental toll that this has taken on our lives has been greater than any other issue we have faced. A large part of this toll has been the ethical considerations and the inadequacy of Christian literature to address the depths of the questions that are brought up when you have to seriously consider IVF as your only option to have biological children. Few people were willing or able to engage with and work through the depths of the questions we had. We spent hours and hours talking it out with each other, reading scientific journals, and questioning doctors on the intricacies of every step of IVF. If you are interested in any of the journals and don’t have access, let me know and I can help.
Below I hope to outline the specific ethical considerations we faced when considering IVF through a Christian worldview and the perspectives that we have come to that give us peace around our decisions. The lessons we learned have been hard-earned, through tears and arguments, and days upon days of learning. Even after all this, I recognize we may still be wrong concerning specifics that I will outline below. IVF is a changing scientific field and is advancing daily. I’m not an embryologist, this isn’t my life's work, but it is important to me. As such, I invite conversation, comments, or emails where you have questions, corrections, or challenges. More than that I hope the specifics below serve as a launching point for couples that must face this challenge, or those that wish to truly understand the challenge better to support friends or family facing infertility. We have come to a place that we believe gives us hope for biological children while honoring the ethical considerations we have as followers of Christ. What is written here focuses primarily on the technical aspects that are not well covered in current Christian literature. I recognize that there are existing sources for some of the bigger-picture moral questions around fertility treatments, what God says about life, and us as reproductive/creative beings. I may have additional writing on that in the future.
The Elephant in the Room
The single largest ethical consideration when IVF is approached is the most obvious. The process of IVF involves the creation of embryos, and in doing so you open the possibility for embryos to be lost or discarded, whether intentionally or unintentionally. From our perspective, we would have to disregard our belief that life begins at conception to be ethically okay with discarding embryos. That seems to make the idea of IVF untenable from the start for us and many Christ followers. This led us to our first conviction: For any embryos that we create, we will do everything in our power to give them every chance of a viable pregnancy.
The sections below are written in a way meant to outline several challenges to the above conviction that we were forced to consider. From the very start, the simplified statement that is often parroted - “Life begins at conception” - falls short of the complexity of the issue.
Challenge 1: Grading of Embryos
In the process of embryos being created, eggs are manually inseminated for fertilization to occur. If the egg accepts the sperm’s genetic material, then fertilization occurs and the embryo begins growing by splitting into two cells. We would consider this to be the beginning of life.1 However during the incubation period (Day 1-Day 5), an embryo may stop growing anytime. Embryologists typically check embryo status on Day 5. How do you determine if an embryo is alive from fertilization until transfer?
The challenge this brings to our conviction of IVF is simple: if life begins at conception, which we believe to be after fertilization has occurred, then if we are creating embryos that die between days 1 and 5, are we being poor stewards of potential life?
After sperm and egg are successfully combined and fertilization occurs, embryos are grown in conditions that are nearly exactly the same as they would be in the female reproductive system. The standard for most clinics is that they will either pull embryos on day 3 or day 5. Some will continue to culture embryos that show active cell division on Day 5 up to Day 6 or 7. Our clinic will culture out to day 7, and we think this is an important consideration to give still-growing embryos every possible chance. After the culturing is complete, they grade embryos based on the visual components of the embryo. If you are interested, a good visual descriptive resource is here: (https://advancedfertility.com/fertility-gallery/blastocyst-images/)
One major thing to clarify at this part of the process is that some clinics will use different grading systems or grade slightly differently. There are standardized methods, but it’s important to understand the specifics of how any individual clinic approaches grading. The above link has information and terminology that can assist in your understanding of terms if you are interested. Of particular note for us was a description given of a “D” grade embryo. “D” grade embryos are occasionally created in the IVF process and are generally described as having a greater than 50% of their ICM (Inner Cell Mass) or TE (Trophectoderm) being fragmented. They have the appearance of blastocysts, but the cells that make up the blastocyst are more than 50% dead, or the cells that are expected to be a part of the embryo simply aren’t there. Most clinics will not transfer D grade embryos. While this initially gave us pause, over time we could not find an instance of a D grade embryo resulting in a live pregnancy. After working through the definition through a conversation with our embryologist and a few papers (https://academic.oup.com/molehr/article/2/2/93/1007067), we came to the understanding that even though it may have the slight appearance of a blastocyst, the cells inside are dying or already dead. It is in the process of cellular death and can not be considered a viable embryo.
Embryos below a C grade either in the TE or ICM show effectively no cellular growth in those vital areas. While grading can be considered a little subjective, good embryologists can tell the difference between the grades as shown by the birth rate correlation from embryo grading. For a helpful site on grading, see https://www.remembryo.com/embryo-grading/#Blastocyst_embryo_grading_Day_5_grading.
Grading is something to know about because grading has a direct correlation to the clinical pregnancy rate and live birth rate.
https://pubmed.ncbi.nlm.nih.gov/33565291/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5987494/

In general, 66% of eggs will actually fertilize and begin the culture process. Of those embryos, 50% that are cultured will make it to the blastocyst stage, which is the optimal stage for embryo transfer. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6504986/) As an example, if you started with 4 eggs, statistically 2 or 3 will fertilize, and one or two would make it to the blastocyst embryo stage. So what happened to the 1 or two embryos that fertilized and did not make it to the blastocyst stage?
The clinical term is that the embryo’s growth has arrested; the simple way to think about it is that the embryo dies somewhere between day 1 and day 5. This is not a unique occurrence to IVF. It is common for a percentage of natural conceptions to be lost, though the percentage is debated primarily because it is very difficult to measure, the best range estimates I could find are in the 10-40% range prior to implantation. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5443340/) There’s reason to believe it may be higher as well, in the range of 50-75% This is reasonably comparable to the theoretical 50% loss rate from fertilization to blastocyst stage in IVF. To put it simply, if you are a couple that does not have issues with fertility, you have likely had several eggs that were fertilized and died without you even knowing it.
This was an important part of our ethical considerations. It showed that the medical procedure of IVF can be able to overcome infertility, which we understand to be a result of a fallen world. IVF statistics show a reasonable parallel to the natural world in terms of percentage loss of embryos after fertilization. In addition, the monitoring and priming of the female reproductive system prior to an embryo transfer optimize the conditions for implantation.
In regards to the initial question “How do you determine if an embryo is alive from fertilization until transfer?”, we determined that if the embryo grew to a blastocyst with greater than 50% of its cells actively dividing, it was alive and should be transferred. The percent of cells that exist and are actively dividing shows the directionality of the embryo; if the majority of cells are not actively dividing, the embryo is moving towards complete arrest. We also found that it’s likely that the growth of embryos and the loss rates around IVF are similar to attempts to naturally conceive.
Challenge 2: Genetic Embryo Testing.
Without getting too much into the weeds on the three types of pre-implantation testing, PGT-A testing is a fairly recent test in the IVF world that has become increasingly widespread. The effectiveness of the test is debated, but the simple description is that it can tell you which embryos should implant, and which will fail to implant. Embryos are biopsied for just a few cells and they are sent out for testing of chromosomes.2 Embryos that are called euploid exhibit low amounts of cells with chromosomal abnormalities. (<20%) Mosaic embryos exhibit moderate amounts of cells with chromosomal abnormalities 20%-80%. Aneuploid embryos have many cells with severe chromosomal abnormalities (>80%). There’s much more to the testing, but that’s the easiest way to describe it. It’s also an incomplete way to describe it, and if you’re interested in the weeds, this paper is an important one to read. It speaks to the arbitrary cutoff points I just described (in %s) and has a more complete view on mosaic vs aneuploid vs euploid. (https://www.fertstert.org/article/S0015-0282(21)00527-6/fulltext) There is an important ethical conversation around eugenics that should be had with the other PGT testing options (PGT-M, PGT-SR) that are available, but it’s outside of what I have ethically considered supporting. We decided not to do PGT-A testing initially because we had no reason to believe that PGT-A was necessary during our first fertilization cycles as we expected a viable pregnancy within our first transfers. Additionally, most clinics will not consider an ET (embryo transfer) of aneuploid embryos and as a standard aneuploids are often immediately discarded. This means you could have an embryo that is seemingly ready to implant when looked at under a microscope with grading criteria, but the PGT-A testing could rule out the transfer if the testing results showed aneuploidy.3 This seemed to violate our initial primary conviction of doing everything in our power to transfer every embryo we create. After three failed embryo transfers, we are PGT testing our two embryos on our third round of fertilization but are requesting to receive the PGT results after the transfer. This gives us valuable insights into whether we are transferring embryos that should implant and are not, without the risk of not being able to transfer aneuploid embryos. This gives us more direction for additional maternal/paternal testing, other treatments to consider, or if it is simply abnormal embryos.
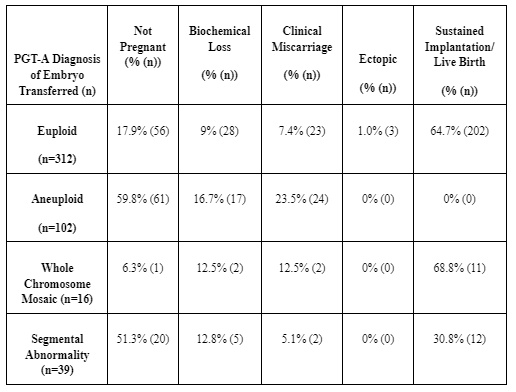
The question I would encourage any person approaching this with a Christian worldview to ponder is this: If a PGT-A test can tell you that an aneuploid embryo will not result in a live birth 100% of the time, should you still transfer that embryo?4* That is one of the many difficult questions we have thought hard about, and one study that is impactful in this consideration for me so far is this one. https://pubmed.ncbi.nlm.nih.gov/32863013/
In a blinded test, all embryos that were tested to be aneuploid failed to sustain implantation and result in a live birth. I present this as a consideration, to help you think critically about what your expectations are of the treatment of embryos. We don’t have an answer to this question yet, as we are still working through it.
Challenge 3: Miscellaneous Concerns
After the embryos are created, there are options to consider when transferring them. For those that have not had to go through IVF or know very little about the process, the first step is an ER (egg retrieval) and usually an immediate fertilization of the eggs, after which the embryo(s) created are either transferred and/or frozen. The egg retrieval is an entirely unpleasant process, with the goal of producing as many mature eggs as possible, usually in the range of 6-25. However, you can end up with zero to as many as 50. The reason for immediate fertilization is often to prevent the loss of eggs, to give the greatest number of transfer-ready embryos, and to know exactly what you have to work with moving forward. By knowing how many embryos are available, it allows you to be more calculated in planning your future steps for success with cost-benefit in mind. In normal IVF cycles, all eggs are fertilized, and however many embryos come from the fertilization are either transferred and/or frozen.
Of all the questions in IVF, one of the most difficult from our perspective is how many eggs to fertilize at one time. Fertilization is (rightly) by far the most expensive part of the whole process. A full IVF cycle from egg retrieval through first embryo transfer can be $15,000-$20,000 and varies widely based on needs and insurance coverage. Insurance rarely covers fertility treatments in general.5* Of that range of cost, embryology fertilization services make up about $7,000-$9,000. This implies a significant financial burden if you decide to do multiple rounds of fertilization using frozen eggs. We decided morally that we were not comfortable with fertilizing all eggs immediately, and counted the financial burden as worth it to have a clear conscience at the get-go. Subsequent transfers can be in the range of $2,000-$3,000 additionally.6*
From our perspective, the fertilization of all eggs was not a responsible approach for us to take, keeping our first conviction in mind of being obligated to every embryo we create. Our egg retrieval collected 30 eggs, of which 18 were mature (usable for IVF). We immediately fertilized 4 eggs and froze the other 14 mature eggs.7 Our initial decision of fertilizing 4 eggs was driven by several factors. The primary apprehension is creating more embryos than children we desire. For example: If all 4 eggs fertilized and became embryos, no matter how unlikely, we commit to transferring them with the intention of viable pregnancies.8 Additionally, we were unsure of how successful our initial egg retrieval, fertilization, or transfers would be, so we erred on the cautious side of statistical possibilities (referenced in Challenge 1), knowing that more than two embryos would be unlikely.
Before starting IVF, patients are required to sign legal documents regarding the disposition of frozen embryos - i.e. what happens to your embryos if you die. This forces patients to consider worst-case scenarios which leads us to our next apprehension: an unforeseen circumstances where Sarah is unable to carry out a pregnancy with remaining frozen embryos (e.g. cancer, hysterectomy, multiple cesarean deliveries, etc), or tragedy strikes and we or Sarah dies unexpectedly. These scenarios are unlikely but pose a very real threat to the well-being of human life embryos that we are obligated to protect. Our fertilization related decisions were intentionally made to avoid surrogacy or contributions to the embryo adoption bank; it has no shortage with 600,000 embryos waiting for adoption. Just as one plans a will or contingency plans for children in the case of parental death, we also believe it is wise to plan with the same vigor and love for frozen embryo children who are not yet born. We ought to plan in a way that affords them the best outcome with their best interest in any tragic scenario.
Per the logic above, we believe the first and most important step is reducing the risk of having frozen embryo(s) awaiting transfers for long periods of time by limiting the number of embryos created and frozen at any given time. Second, if we learned that Sarah is unable to carry out a pregnancy or Sarah unexpectedly dies, we agreed that the next best option would be to perform a transfer with a surrogate, ideally someone we know and trust. We would rather work with a surrogate than never transfer this embryo or donate this embryo for adoption. Third is the case of the unexpected death of both of us. We had frank conversations with trusted family and friends who have expressed willingness to care for our embryos as we would. In the case of more unforeseen circumstances, we have confidence that they would lovingly and responsibly work with a surrogate or lastly match the embryo(s) to an adoptive family. Our intention is that these embryos will not be frozen forever or discarded and will always have someone protecting them.
To be perfectly honest, in hindsight it was the wrong decision from a purely practical standpoint. We have gone through three fertilization rounds and three transfers over the span of one year and have not had a viable pregnancy yet (though we have had two chemical pregnancies). I say this as a reality check to those that often issue a blanket condemnation on the creation of many embryos through a fertilization cycle as irresponsible. The factors involved are intricate and multifaceted, and unless you are actively engaged in the process you likely have a limited understanding. It really is a case-by-case basis decision. I don’t regret our decisions, we have moved forward in a way that is in line with our beliefs, and I would advise any Christian to proceed with the same caution. I would advise any Christians considering IVF to fertilize eggs in a way that will leave them with no more embryos than they are willing to transfer for the intention of pregnancy. It’s not a decision to take lightly, quickly, or emotionally. It should involve much prayer and serious thought. At the same time, we have had to face the reality that speaking purely from a results standpoint our decisions have made our lives significantly harder.
Challenge 4: Embryo Freezing
After embryos are created they are frozen through a process called vitrification and kept until a future transfer date. Some people choose to do a fresh embryo transfer depending on their body's response to the egg retrieval medicine. Freezing embryos comes with a non-zero risk that the embryo will be destroyed in the process. This one for me seems fairly simple. From this study, embryos frozen and warmed in vitrification cycles after 2015 had a 2.5% loss rate after warming. (https://link.springer.com/article/10.1007/s10815-021-02284-0)
There is a low risk of losing an embryo to the freeze/thaw process, and even so, the risk of embryo loss could be greater with transfers associated with OHSS (ovarian hyperstimulation syndrome) (https://pubmed.ncbi.nlm.nih.gov/24163797/) I don’t believe the freezing of embryos should be outlawed, as is the policy in Germany, because very simply it does not allow for optimal treatment of the patient or embryo. Without optimal treatment, you will likely destroy more embryos by banning freezing than you would by allowing it. I also do not believe that the risks posed to the embryo by freezing are meaningful enough to outright condemn IVF as a practice, but it should be understood and considered by those undergoing the procedure.
Questions to consider:
If you are concerned with the risk of the destruction of embryos in IVF, consider the risks around the destruction of viable embryos through spontaneous abortion in natural conceptions. Consider if you work(ed) to mitigate those risks prior to attempting to have your own children. Do you understand what those risks are? Have you also considered the implications of levying criticism toward percentage destruction rates of embryos in IVF as compared to natural conception? For example, if a couple was trying to conceive, did they do laparoscopic surgery prior to attempting conception to look for endometriosis which can cause implantation failure of embryos? Did they have a saline sonogram to evaluate the uterine cavity for endometrial conditions? Did they complete an evaluation of your fallopian tubes to look for Hydrosalpinx, which will also cause implantation failure? Did they consider a hormone panel to ensure optimal conditions for an embryo to implant and for a sustained pregnancy? Are the conditions of the female reproductive system monitored and primed intensely for the entire menstrual cycle leading up to possible implantation? Would you advocate for IVF as the main method of conception if it was proven to be a safer method than natural conception for lessening the destruction of embryos compared to natural conception? All these questions become important to consider and answer especially if the position you take is that fertilized embryos are inherently life before implantation.
Conclusion regarding our first conviction:
We can be effectively cautious in our approach to embryo creation to mitigate the risk of discarding life. There is no scenario, IVF or otherwise, that will prevent the destruction of viable embryos 100% of the time. IVF is a comparative method to current spontaneous abortion rates that occur in natural conception and most cases will not have a known higher destruction rate of embryos if done with patience and care specifically regarding the pace of embryo creation.
Many of the clinical questions above will be considered irrelevant if you find IVF to be an immoral process based on underlying moral issues. I will work to cover those moral issues in a separate post if there is interest.
Some Christians believe conception to mean the moment of implantation. We believe the currently available information points to conception being at the moment of fertilization when life begins.
PGT-A testing has complexities regarding different thresholds used for the determinations of euploid, aneuploid, and mosaic. PGT-A testing is mainly screening for missing or extra whole chromosomes in the embryo to determine the status.
If you desire to do PGT-A testing, while most clinics will not transfer aneuploid embryos, some clinics will transfer aneuploid embryos sent from other clinics if desired. Most clinics will transfer mosaic embryos after genetic counselling is provided.
There are risks involved with any pregnancy or transfer. If a test can show that the aneuploid embryos have no chance of live birth and significantly higher miscarriage rates, is it moral to accept the risks of the transfer to the mother? Some clinics will transfer aneuploid embryos, but PGT testing can also point to conditions such as mosaic trisomies (such as 13 or 21) that no clinics will transfer due to legal liabilities.
Insurance will often cover the diagnosis of underlying treatments, but not treatment. Costs are highly variably dependent on prescriptions, monitoring, travel, and personal choices like PGT or patient testing. Most insurances cover little to no fertility treatments like IVF.
While not the norm, many couples face multiple IVF rounds (retrieval, fertilization, and transfers) to achieve a live birth. Some couples are unable to have a child through IVF despite several rounds and great sacrifice.
The loss rate of freezing eggs is around 20%, although we experienced a 0% loss rate of our frozen eggs. In our opinion, the consideration of lost eggs as part of a fertilization cycle does not hold weight to the ethical issues we have with overproducing embryos.
There is a practice in IVF called Compassionate Transfer which transfers an embryo at a sub-optimal time in a woman's cycle in order to give the embryo a chance at life, though a very slim one. We do not advocate for this method.
Your wife posted this link on my Instagram. I’d be happy to engage with you on this topic. I find your ethical analysis lacking and thin. Unfortunately, there are many people writing seriously about this topic that you are unaware of. Oliver O’Donovan’s Begotten Or Made is excellent. Prof. Matthew Anderson at Baylor has an excellent book out. Paul Ramsey. Gilbert Meileander. Many others including myself have been writing and speaking and doing research on assisted reproduction and infertility.
Thank You for your reseach, faith and analysis. My husband and I found this very helpful. I value your insight because you have actually experienced infertility. As you pointed out in your discussion with a commenter, it takes a very sacrificial love (Agape) to do the shots, mood swings, testing, costs, ups & downs etc. of ART. It is very difficult to find an analysis that doesn't just make blanket statements and speak in ideology. We are complex cases working with limitations in finances, health and time. We have to work within policy and procedures set forth by insurance, medicine and practitioners. God has brought us to this place and now we must know how to proceed. No one comes to IVF without first despertly crying out to God for the easy way to conception to work. It is the most natural & Holy thing in the world to desire to have Children. They are a blessing and mirror of the relationship of God-the-Father and Jesus. May God Bless Your Family!